

Sternoclavicular Joint Reconstruction
Sternoclavicular Joint Reconstruction
Sternoclavicular joint (SCJ) dislocations are uncommon and only account for 2 – 3% of all dislocations of the shoulder girdle. Most dislocations occur anteriorly while only 5 to 27% occur in a posterior direction. Anterior dislocations often do not require any acute treatment while posterior dislocations will require either closed reduction or surgical stabilization due to the proximity of vital structures posterior to the sternum. In the setting of persistent sternoclavicular instability, a variety of methods have been described for reconstruction including local soft tissue repair or augmentation with synthetic material, ligament reconstruction with autograft or allograft or tendon transfer. My preference for reconstruction is a single loop allograft reconstruction which we have reported excellent functional outcomes and stability. (Tashjian's Sternoclavicular Joint Reconstruction Outcomes Manuscript)
Anatomy
The sternoclavicular (SC) joint is a saddle-shaped that is the primary connection between the arm and the rest of the body. The SC joint includes the clavicle which articulates with the manubrium of the sternum and the superior surface of the first rib. Structurally, the articulating surfaces of the SC joint are separated by an articular disc like the acromioclavicular joint. The posterior sternoclavicular ligament provides the primary anteroposterior stabilization of the SC joint. It is a ligament that extends from the posterior aspect of the sternal end of the clavicle to the posterior aspect of the sternum. The anterior sternoclavicular ligament also stabilizes the SC joint and prevents elevation of the clavicle. This ligament joins the medial end of the clavicle and the top edge of the sternum at the joint. The costoclavicular ligament anchors the clavicle to the first rib and is the other primary restraint. The other structures near the SC joint which are important include the great vessels off the heart as well as the trachea and esophagus. A posterior dislocation can place these structures at risk and it why it is important to surgically treat a posterior dislocation. It is also why we perform all SC joint surgery with a thoracic surgeon partner in the operating room who is present during the entire duration of the procedure as an assistant.
Mechanism of Injury
Direct trauma is the most common injury mechanism. Anterior dislocations occur from blows in an anterolateral direction and are more common. Posterior dislocations occur from blows in a posterolateral direction and are less common. Some patients present with atraumatic initiation of symptoms and swelling. These patients typically do not have instability but rather have arthritis at the SC joint. Treatment of arthritis at the SC joint is similar to arthritis at the AC joint which includes NSAIDs, rest, ice, injections and sometimes partial medial clavicle excision for persistent symptoms. No ligament reconstruction is needed in these patients.
Symptoms of an Unstable Sternoclavicular Joint
Symptoms of an unstable sternoclavicular joint include pain and feelings of instability at the SC joint. Pain or instability is worsened with overhead activities and cross body motions of the arm.
Physical Examination and Imaging to Diagnose an Unstable Sternoclavicular Joint
Physical examination of the medial clavicle includes palpation to identify pain at the SC joint. Instability can often be reproduced by manipulating the clavicle which recreates symptoms or bringing the arm into a cross body position. Special xrays can be helpful (serendipity view) although often times a CT scan and MRI is required to evaluate the position of the clavicle with regards to the sternum as well as to define the state of the ligaments at the joint.
Treatment
Anterior or superior SC joint instability can often be treated nonoperatively initially as it does not present a life-threatening problem. Many patients can tolerate an anterior dislocated SC joint and don’t require surgery. Activity modification is typically the only nonoperative treatment that works. All posterior dislocations will require surgical treatment. Initial closed reduction under anesthesia can be performed for a traumatic posterior dislocation. If the posterior dislocation remains persistently unstable after reduction, if a closed reduction is not successful or if an anterior dislocation remains persistently unstable then a reconstruction of the ligaments can be performed.
Surgical reconstruction is performed in the hospital and can be done as an outpatient. The surgical is done in combination with a thoracic surgeon who is present for the entire procedure. A tunnel is created in the sternum and another in the clavicle and an allograft hamstring tendon is then looped between the tunnels and tied recreating the ligaments. A variety of reconstruction techniques have been described including a figure of eight construct. Limitations of the figure of eight technique include the requirement for 4 smaller drill holes (2 in the clavicle and 2 in the sternum) which may be challenging especially in smaller patients or with compromised bone stock. We use allograft instead of autograft as autograft requires a separate incision and potentially increased morbidity. A simple loop reconstruction using allograft is a simple, less morbid technique especially in cases of smaller patients or limited bone stock. I have evaluated my patients using this technique and have shown excellent functional outcomes and stability at long-term. (Tashjian's Sternoclavicular Joint Reconstruction Outcomes Manuscript)
Surgery is typically outpatient where patients will come in and go home the same day. They may need to stay one night. They will be treated postoperatively with an interscalene cathether placed under ultrasound by our anesthesia pain specialists as well as oral medication. Patients will be in a sling for 6 weeks during the daytime and nighttime. The dressings may be removed at 5 days and the wounds can get wet in the shower at that time. Patients will take the sling with a pillow off, place the arm in another simple sling during showering, let the water run over wounds without soaping or scrubbing and then pat dry the shoulder and then place the arm back in the sling with a pillow. Washing under the armpit is allowed. For the first 6 weeks, patients will be doing only elbow wrist and hand range of motion. At 6 weeks, patients may discontinue the sling and start using the arm for everyday activities with no lifting over 5 lbs. Stretching with therapy will continue. At 12 weeks, strengthening with therapy will start and the patient may lift up to 20 lbs. At 4.5 months, the patient will be able to lift up to 40 lbs and at 6 months return to all activities. There will be continued improvement in range of motion and strengthening for up to 12 months after surgery. Return to sport includes walking on the first postoperative day and stationary bike at 2 weeks. Running and jogging can start at 6 weeks. Swimming in a pool and road cycling can start at 3 months. Golf and tennis can start at 5 months. All other contact sports may be initiated at 6 months postoperative.
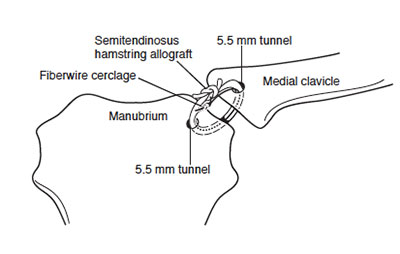
Figure 1 ‐ Diagram of sternoclavicular reconstruction using a looped allograft



Figure 2 ‐ Skin incision (left picture); Drill holes in clavicle and sternum (middle picture); Hamstring allograft passed from the through sternal tunnel (right picture)


Figure 3 ‐ Hamstring allograft passed through clavicular tunnel (left picture); Completed reconstruction (right picture)
You will need the Adobe Reader to view and print these documents.




